1997 Dodgen Lecture
Sandra B. Garofolo
Department of Professional Services
©Amgen Inc., Thousand Oaks, CA 91320-1789
The tools of biotechnology are creating medical breakthroughs. Researchers are constantly discovering and applying new ways to use human proteins to treat and prevent diseases that in the recent past were considered incurable. This program will focus on some of the basic definitions, applications, and clinical issues of biotechnology as they relate to Amgen and the treatment of patients with chronic renal failure.
The origins of biotechnology date back thousands of years to the time when humans shifted from a life of nomadic hunting to one focused on perennial agriculture. The earliest use of biotechnology took place at this time when these people developed the fermentation process by adding yeast to crude mixtures of target foodstuffs and nutrients in clay vessels. These early agricultural scientists adjusted the nutrients, the environment, and the fermentation time to produce a wide variety of tasty products, including bread, wine, cheese, and beer. This may be considered the oldest, and the noblest, use of biotechnology of which we are aware.
There are a variety of definitions of biotechnology. The simplest and broadest one is as follows:
The use of tissue cultures, living cells, or cell enzymes to make a defined product.
Modern biotechnology is, in fact, an integration of a number of scientific disciplines and tools, including microbiology, immunology, genetics, molecular biology, biochemistry, and engineering, for the purpose of producing useful products. The application of these tools to patient care is referred to as biotherapy. This term is used to describe the employment of biotechnology products for the diagnosis and/or treatment of disease. This includes the administration of proteins or nucleic acids for the following: (1) correcting deficiencies of endogenous compounds, (2) enhancing natural physiologic processes, and (3) blocking dysfunctional proteins or nucleic acids.
Recombinant DNA technology, in its most basic form, involves processes that take a strand of foreign DNA that encodes for a protein normally expressed in small quantities, and ultimately produce this gene's protein in large enough quantities for commercial production (Figure 1). The first step typically involves the isolation of the strand of foreign DNA--for example, a human gene--that encodes for the protein of interest. This genetic material may then be inserted into the DNA of a host cell which will act as the factory for the protein production. Different kinds of cells used for host cells include certain yeast, bacteria, and mammalian cells that are capable of being quickly and easily manipulated.
Plasmids are useful structures in recombinant DNA technology (Figure 2). They are circular pieces of bacterial DNA that are not part of a chromosome and are not essential for the cell's function. They easily accept and reproduce foreign strands of DNA, and are used as vectors to carry DNA to host cells for replication. A large number of plasmids could be inserted into the host cell and cause the foreign DNA to be amplified many times as the cells reproduced, yielding large amounts of the inserted piece of foreign DNA, and ultimately, the protein for which it encodes (Figure 3). The plasmid must be cut open with restriction enzymes, forming a gap in the plasmid ring. The desired gene is then inserted or spliced into the break of the plasmid and "pasted" with the aid of the enzyme DNA ligase.
The plasmid, now carrying the foreign DNA sequence encoding for the desired protein, acts as a vector and is then transferred back into the host cell where it will be replicated. This process is called transformation (Figure 4). Host cells, placed in an appropriate growth medium with a carefully controlled nutrient mixture and environment, produce millions of genetically identical cells which replicate the inserted gene with all of the host's original genetic material (Figure 5). This process, in which a specific DNA fragment is isolated and propagated in large amounts, is referred to as cloning. Ultimately, the desired protein is expressed and secreted in large quantities into the growth medium.
For commercial production, the process begins with a small amount of inoculum (containing billions of cells) being transferred to fermentation flasks and ultimately to the final site of cell growth (examples, fermentors and roller bottles) containing the appropriate culture medium and nutrients. Next follows a complex series of steps involved in the processes of cell culture, purification (techniques include sterile filtration and column chromatography), and formulation of the final product (by the addition of buffers and stabilizers to give the biological a maximal shelf life).
There are many steps involved in the research and development of new biologicals that span across the period from discovery to commercial availability. Discovery of biologicals focuses on the disciplines of molecular biology and biochemistry to tap into the natural human cellular processes that can provide a wealth of protein products. After a biological is discovered, it must go through pre-clinical research and development, including animal testing and work on formulations and manufacturing scale-up. After animal testing, an Investigational New Drug (IND) application is submitted to a branch of the FDA referred to as the Center for Biologics Evaluation and Review (CBER). With the acceptance of the IND, clinical trials follow, which are generally divided into three phases. Phase 1 studies evaluate the safety, metabolism, and pharmacology of the agent in small numbers of normal human subjects. In Phase 2 trials, the efficacy of the drug is tested in small numbers of patients who have the disease that the drug is intended to prevent or treat. Phase 3 studies are conducted in large numbers of patients for the purpose of evaluating safety, effectiveness, and dosage. The Biologics License Application (BLA) summarizes the manufacturing process and the results of clinical testing, and is submitted by the manufacturer to the FDA as a formal request to market the product. After a product receives marketing clearance, there are a number of important post-marketing activities, including: (1) commercial use, (2) additional clinical trials, (3) adverse event reporting, (4) educational program review, and (5) promotional/advertising review.
Now we will switch gears and discuss a class of biologicals, and a specific product in this class, to which Amgen has devoted a significant amount of time and attention. The area of interest is hematopoiesis, and the class of biologicals can be described as hematopoietic growth factors. Although Amgen is involved in ongoing activities looking at a number of cell lineages in this area, for the purpose of this discussion we will concern ourselves with the erythroid (red blood cell) lineage and the hormone, erythropoietin. We will now see how Amgen has used the tools of biotechnology to produce a therapeutic (recombinant human erythropoietin, EPOGEN®, Epoetin alfa) that has a significant impact on the lives of patients with chronic renal failure on dialysis.
To begin we will focus on the historical perspective. In 1836, Richard Bright described anemia as a complication of renal failure. Erslev identified a hormone in 1953 that he called erythropoietin which was responsible for regulating red blood cell production. In 1957, Jacobson proved that erythropoietin was manufactured in the kidney, and in 1977, Goldwasser and colleagues purified human erythropoietin from urine. Fu-Kuen Lin was the first to isolate and clone the human erythropoietin gene in 1983. Clinical trials investigating recombinant human erythropoietin for the treatment of anemia in patients on dialysis were initiated in December of 1985, and the FDA granted marketing clearance for EPOGEN® for the treatment of anemia associated with chronic renal failure on June 1, 1989. Subsequent FDA approval for the treatment of anemia associated with zidovudine (AZT) therapy in HIV-infected patients occurred in December of 1990, and for anemia associated with chemotherapy in patients with non-myeloid malignancies in April of 1993. The most recent indication was approved in December of 1996, and allows for the treatment of anemic patients scheduled to undergo elective, non cardiac, non vascular surgery to reduce the need for allogeneic blood transfusions.
As background we will review some basic physiology. The kidneys are primarily organs of filtration and excretion and are responsible for maintaining fluid balance and removing end-products of metabolism. In addition, they are involved in regulation of systemic blood pressure, regulation of pH, the metabolism of vitamin D, and the regulation of erythropoiesis. This last function will be the main focus of the rest of this discussion.
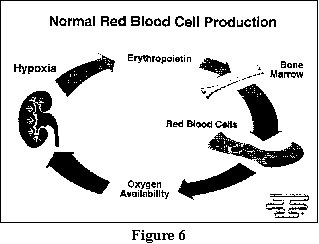
The erythrocyte, or red blood cell, is shaped like a biconcave disc and is responsible for the transport of oxygen and carbon dioxide. The red color comes from hemoglobin, which is a complex of iron and protein that makes the cell capable of binding respiratory gases for transport. In normal humans, red blood cell production is triggered by hypoxia (decreased oxygen content in the blood). During anemia, the red blood cell count is reduced, which results in a lowering of the oxygen content of the blood. This hypoxia is sensed by the endothelial cells of the peritubular capillaries in the kidney, which stimulates cells in the renal cortex to produce erythropoietin (Figure 6). Erythropoietin is secreted into the circulation and travels to the bone marrow, where it stimulates erythroid progenitor cells to differentiate and proliferate into mature erythrocytes. These erythrocytes increase the oxygen-carrying capacity of the blood, thereby decreasing the hypoxic stimulus and the stimulus for erythropoietin production.
The patient with chronic renal failure suffers from a host of debilitating clinical signs and symptoms, including anemia. Uremia affects virtually every organ system in the body. Patients with chronic renal failure often suffer from such problems as lethargy, fatigue, mental confusion, hypertension, edema, gastrointestinal bleeding, and congestive heart failure. Survival for patients with end-stage renal disease ultimately depends on ongoing dialysis treatment or a kidney transplant. For patients who are treated with dialysis, therapy includes dietary and pharmacologic measures in addition to their dialysis regimen.
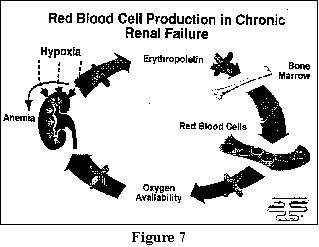
When the kidney is irreversibly damaged, it cannot respond to a decrease in oxygen availability by producing erythropoietin. Therefore, the primary mechanism underlying the anemia of chronic renal failure is an erythropoietin deficiency. Secondary to this lack of erythropoietin, the normal feedback loop is interrupted and anemia ensues (Figure 7). Many additional factors contribute to the anemia of chronic renal failure, including blood loss, iron deficiency, aluminum toxicity, and vitamin deficiencies. The manifestations of this long-standing anemia in patients with chronic renal failure include fatigue, weakness, shortness of breath, angina, intolerance to cold, loss of appetite, insomnia, depression, cognitive impairment, cardiac enlargement, sexual dysfunction, and reduced exercise capacity. Many of these signs and symptoms were previously attributed to uremia itself. They were later found to be secondary to the anemia associated with chronic renal failure and the resultant impaired oxygen delivery to tissues for normal functioning. In the past, anemia of chronic renal failure was treated with blood transfusions and androgen therapy, both with associated risks. However, in 1989 EPOGEN® received marketing clearance from the FDA and has had a tremendous positive impact on the management of renal anemia.
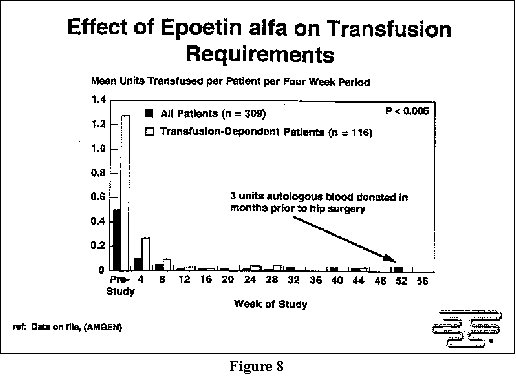
The Phase 3 pivotal trial that evaluated the safety and efficacy of Epoetin alfa was conducted in 333 anemic dialysis patients with a mean baseline hematocrit of 22%. After 12 weeks of therapy with Epoetin alfa, 97.4% of patients responded and achieved a mean hematocrit of 35%. Transfusion requirements decreased dramatically during the initial two months of treatment, and remained so throughout the follow-up period (Figure 8). One patient was actually able to auto donate three units of blood in the month prior to elective hip surgery about a year after the trial began.
There are a number of quality of life improvements associated with the partial correction of anemia in dialysis patients treated with Epoetin alfa therapy. Patients experience an improvement in their overall sense of well-being. They also experience improvements in exercise and physical performance, cognitive function, and hospitalization rates and reductions in exercise-induced myocardial schemia and left ventricular hypertrophy.
To wrap things up, for those of us in healthcare and the sciences who have come up through school and years of technical training and experience, the one application of biotechnology that we reviewed here, the use of EPOGEN® to treat the debilitating anemia in patients with chronic renal failure on dialysis, may seem like the pinnacle of achievement in medical research, a miracle never before thought possible. How can we top the ability to mimic our body's own capacity to manufacture a protein, and to administer that protein to patients to restore quality of life and functional ability, and to improve survival? For those of us who wonder how we can do better, we will end on this story. When Columbus returned to the New World, a crowd of people gathered at the dock to welcome him home and congratulate him on his discoveries. One young boy was unable to see over the crowd, and was lifted onto the shoulders of the man who stood next to him so he could enjoy the scene with the rest of the onlookers. As everyone else cheered in celebration, this little boy looked discouraged and disappointed, and asked the man who was holding him, "Is there anything left to discover?" The boy's name was Ferdinand Magellan.
In conclusion, Amgen is busy trying to identify and develop prospective future products, in a wide variety of therapeutic areas, that are in the process of being investigated. The application of biotechnology to the treatment of patients with chronic renal failure, which we just quickly reviewed, may be just the tip of the iceberg.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}